News & Articles
Browse all content by date.
“For American kids back in 1986, only 12.8% had chronic diseases. That number has grown to 54% among the vaccine generation (those born after 1986) in lockstep with the expanding vaccination schedule.” – Robert F. Kennedy, Jr
Definition of Generation V: that group of American children and young adults that were born after 1986, when the US Congress passed a law that made it illegal for parents of childhood victims of Big Pharma’s “unavoidably unsafe vaccines” to sue either the corporations that made the vaccines or the physicians and clinics that injected the vaccines when those vaccines caused deaths, disabilities or either acute or chronic illnesses. Because of this law, there was a predictable, rapid increase in the number of vaccines mandated for infants and children by the CDC, the AAP and the AMA.
(Note: It appears that most journalists - even healthcare journalists - that write for news outlets that accept advertising money from pharmaceutical/vaccine corporations are either vaccinology-illiterate (and therefore have to make use of the pro-corporate dis-information provided by the Big Pharmaceutical corporations or the unbalanced, pro-over-vaccination mis-information provided by the CDC, the AAP or the AMA) or they are forbidden to write the unwelcome truths about the well-documented toxicity of the cocktails of vaccines that are routinely injected into America’s infants. (See the chart below.)
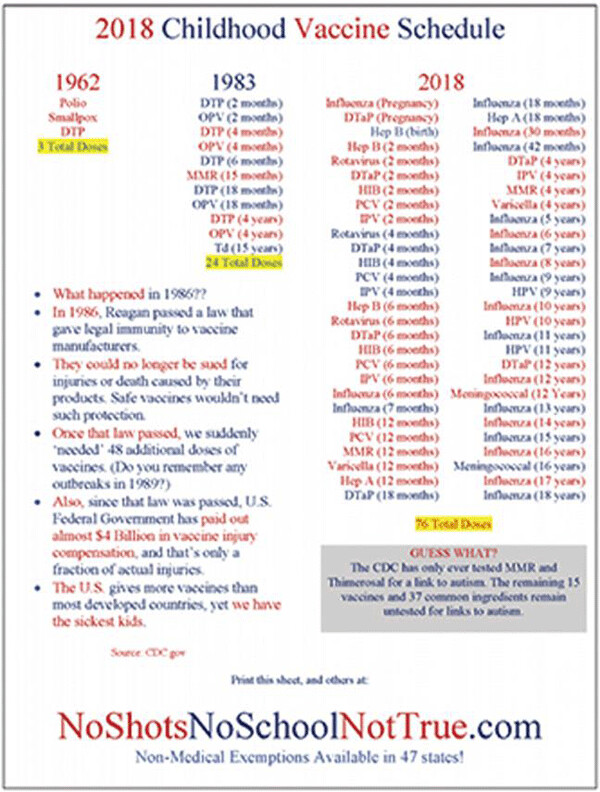
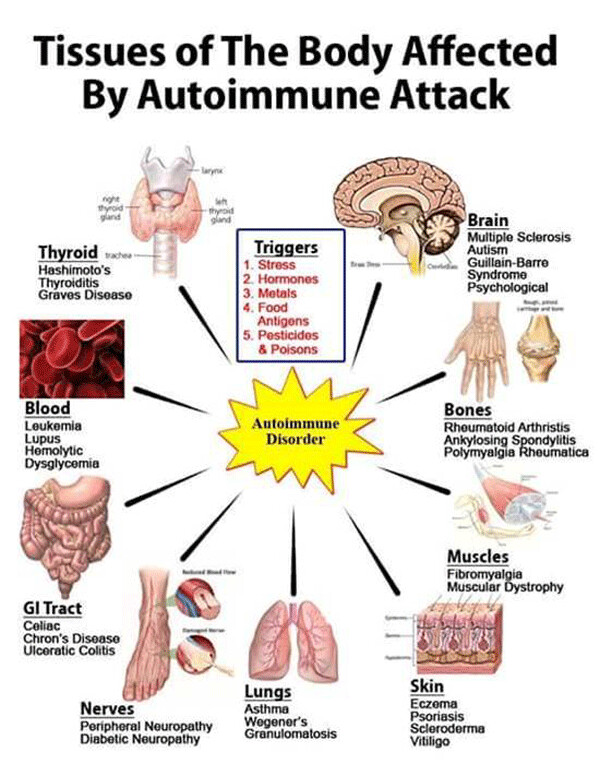
Routinely omitted from healthcare reporting are the thousands of heart-breaking stories from parents of vaccine-injured, disabled or killed infants and children (see a list of some of the vaccine-induced autoimmune disorders below and see a list of some of the industry-acknowledged, vaccine-induced physical and neuropsychiatric disorders in last week’s Duty to Warn column at http://duluthreader.com/articles/2019/10/10/18412_dooming_californias_generation_v) Also never written about are the many well-documented, science-based studies concerning the origins of the epidemic of vaccine-injured infants and children that has occurred since 1989, when the CDC’s and AAP’s vaccination schedules mushroomed (see chart below). Revealed below are some of the correlations between vaccines and vaccine injuries that should give pause to any conscientious, open-minded human being (including physicians) that can no longer deny the evidence of the dramatic increases in the numbers of infant deaths and chronic childhood illnesses since America’s over-vaccination schedule for infants began in the research labs and marketing departments of multinational pharmaceutical corporate entities.
The rise in life-long chronic illnesses is occurring among America’s population of fully vaccinated infants and children. Such illnesses are very rarely seen in the minimally-vaccinated or unvaccinated children. (See the evidence for this statement in the book co-authored by Dr Mayer Eisenstein and Neil Z. Miller that was titled “Make an Informed Vaccine Decision for the Health of Your Child”.) There is a virtual epidemic of chronic autoimmune disorders that include insulin-dependent diabetes, rheumatoid arthritis, lupus, Graves’ disease, celiac disease, inflammatory bowel disease, multiple sclerosis, acute flaccid myelitis, childhood neurological/behavioral disorders (including autism spectrum disorders, ADD, Tourette’s, etc, etc) and allergic disorders (asthma, peanut allergies, etc, etc). The information below is just an introduction to the problem. There are many sources of information that are never revealed in publications that are approved by the CDC, the FDA, the Mainstream Media, the AAP, the AMA, your local hospitals or clinics, Big Pharma corporations, Wall Street, etc, etc.
Part of the solution to the epidemics noted above has to begin with unbiased health education of parents, healthcare workers and healthcare journalists. Then, parents who are fully informed about the ingredients of the vaccines and the risks and benefits need to make an informed decision about which of the multitude of vaccines makes sense for their child. After all, it is the medicolegal right of parents to know about the potential toxicity from ingredients such as mercury, aluminum, formaldehyde, etc that are dissolved in the FDA-approved (but untested for long-term safety), intramuscularly-injected vaccines.
By the way, it is important to understand that the metallic aluminum adjuvanted molecules that get injected into muscle or subcutaneous tissue are never excreted (indeed they increase with every vaccination) because the body’s macrophages [white blood cells] ingest the “foreign bodies” in the body’s tissues and then they deliver them to lymph nodes, the thymus gland, the bone marrow and even across the blood-brain barrier into the brain.
(More information on the ingredients in specific vaccines can be found at: https://img1.wsimg.com/blobby/go/9308dbb4-9d98-4088-a485-9de1adb176c4/downloads/1cpsjgbtg_694234.pdf?ver=1555382968098.) Please read carefully the following important article by Robert F. Kennedy Jr’s Children’s Health Defense Team and be sure to read some of the other equally-important articles at their website (https://childrenshealthdefense.org/news/infant-and-child-mortality-in-the-u-s-nothing-to-brag-about/).
Infant and Child Mortality in the US—Nothing to Brag About
by the Children’s Health Defense Team – September 26, 2019 (1410 words) https://childrenshealthdefense.org/news/infant-and-child-mortality-in-the-u-s-nothing-to-brag-about/ Note: This article primarily focuses on infant mortality; a follow-up article will discuss child and adolescent mortality in greater detail. The United States spends over $230 billion annually on children’s personal health care, representing about 8.4% of total U.S. health care spending. Spending jumped by 56% between 1996 and 2013—with some of the increase likely covering vaccine program costs that began “dramatically” escalating in the 1990s—but these substantial outlays are not translating into a rosy health picture for American children. Instead, leading child health indicators seem to be giving new meaning to the phrase “geography is destiny.” International comparisons show that the U.S. has ranked lowest among twenty developed nations for child mortality since the 1990s and currently ranks behind 55 other countries worldwide for infant mortality. The U.S. also lags behind other developed countries in terms of the rate at which infant mortality is declining—in fact, infant mortality due to prematurity or low birthweight began trending upward in th late 1980se. At present, U.S.-born children are 76% more likely to die before their first birthday than infants in other wealthy nations—with 1 out of every 270 American babies dying in their first year of life as of 2015. Thus, from infancy on, young Americans are confronted with the challenge of beating terrible odds.
Welcome to the Profit-minded Corporate World of Wall Street and its Big Vaccine, Big Pharma, Big Medicine and Big Government Sectors
Considering deaths that occur on the first day of life, it is sadly noteworthy that more American newborns die the day they are born than in any other developed nation. Globally, 68 other countries have a better standing than the U.S. in terms of newborn deaths. Many of these tragic deaths are related to the higher percentage of premature births that occur in the U.S. compared to other developed countries. Could this have anything to do with the United States’ non-evidence-based administration of vaccines during pregnancy, and influenza vaccines in particular? Babies born to women who received (mercury-containing) flu shots during pregnancy are at greater risk of preterm birth as well as low birthweight and fetal death. Internationally, researchers have objected to across-the-board influenza vaccination of pregnant women in the absence of “strong and consistent” randomized clinical trial evidence—and in the U.S., no vaccines have ever been approved by the Food and Drug Administration (FDA) “specifically for use during pregnancy to protect the infant”—yet the CDC continues to tell pregnant women that flu shots are safe. Black babies in the U.S. are at particular risk of dying in their first month or year, with a 2.5 to 2.8 times higher risk of mortality compared to white infants. Common causes of excess mortality in black infants include perinatal conditions and sudden infant death syndrome (SIDS).
Running the “First Year of Life” Vaccine Gauntlet
When it comes to post-neonatal deaths of American infants—those that occur between 28 days and one year—SIDS is the leading cause. By definition, SIDS refers to death in a “seemingly normal, healthy infant under one year of age” that is both unexpected and unexplainable, but again, there is mounting evidence that at least some of the phenomenon may be “medically induced” through vaccination. Without even counting the vaccines administered prenatally, American infants receive more vaccines in their first year than infants anywhere in the world. Many of those vaccines are administered in bundles at well-baby visits around two and four months—exactly when nine out of ten SIDS deaths occur. U.S. researchers have largely ignored the important question of a potential SIDS-vaccine connection. However, European investigators have examined the issue as it pertains to some combination vaccines. For example, a study by Italian researchers described the case of a three-month-old infant who died within 24 yours of receiving the Infanrix hexa vaccine manufactured by GlaxoSmithKline. (The six-in-one vaccine includes antigens for diphtheria, tetanus, acellular pertussis, Haemophilus influenzae type B, poliovirus and hepatitis B.) After examining clinical data, postmortem findings and immunohistochemical and laboratory analyses, the investigators concluded that “acute respiratory failure likely due to post hexavalent immunization-related shock was the cause of death.” Recently, an independent Italian research group studied the chemical composition profile of Infanrix hexa and was surprised to find that it showed zero evidence of the six antibody-inducing antigens that the vaccine is supposed to provide. Instead, the hexavalent vaccine contained numerous chemical contaminants and toxins, bacterial peptide toxins as well as an “insoluble and indigestible macromolecule” unrecognizable by any protein databases—in short, “a compound with an unknown and unpredictable toxicity and efficacy.” Another set of Italian researchers conducted histological examinations of over 100 young SIDS victims for whom detailed clinical and environmental information was available; in 12% of the cases, the SIDS deaths occurred within one to seven days of hexavalent vaccination. The authors deemed it plausible that “vaccine components could have a direct role in sparking off a lethal outcome in vulnerable babies.” Considering precisely this question of “vulnerable babies,” a group of Spanish researchers reviewed clinical and surveillance studies of hexavalent vaccination in infants born premature or low birthweight. Although casually dismissive of most vaccination risks in this delicate subpopulation, the authors nevertheless reported that 13% to 30% of “medically stable” babies with a history of prematurity or low birthweight had experienced an adverse cardiorespiratory event (cessation of breathing or abnormally low heart rate) following just one dose of hexavalent vaccine.
Back in the US
In the US, the Centers for Disease Control and Prevention (CDC) employs evasive semantics to avoid too many troubling questions about the causes of SIDS. It does so by lumping SIDS under the broader three-pronged umbrella of “sudden unexpected infant deaths” (SUID), which separates SIDS events from deaths from “unknown causes” and “accidental suffocation and strangulation in bed” (ASSB). As a result, the agency likes to claim that SIDS rates fell in the 1990s and have remained stationary since then. However, a 2006 analysis by some of the CDC’s own researchers showed that most of the apparent decline was an artifact of the CDC’s changes in cause- of-death classification from SIDS in favor of “cause unknown/unspecified” and ASSB. Other factors point to considerable underreporting of SIDS deaths, including reporting anomalies, the inadequacies of death certificates as a source of complete information and the “complicated” and “convoluted” process involved in creating and registering causes of death for public records. In a surprising concession, the U.S. Court of Federal Claims ruled in 2017 that there was “preponderant evidence” supporting a claim that vaccines “caused or substantially contributed” to a 2011 SIDS death. The court, which has a notoriously high burden of proof, also ruled that the death could not be attributed to non-vaccine-related factors. Unfortunately, the ruling has had no consequential impact on childhood vaccine policies. Au contraire—states like California, New York and Maine are now stomping on the human rights of even the most medically fragile children and sanctimoniously denying that vaccine-related injuries and deaths even occur. Moreover, despite the various studies highlighting hexavalent vaccine dangers, the FDA just saw fit, in December 2018, to approve the U.S.’s first hexavalent pediatric vaccine; Vaxelis, jointly manufactured by Sanofi and Merck, will be made available to the pediatric vaccine market sometime in 2020. With the disproportionately high rates of premature birth, low birthweight, birth defects and other infant health challenges that prevail in the U.S., policy-makers should be acknowledging that vulnerable babies abound. At the same time, they should be taking note of the fact that vulnerabilities are not always apparent and are not the whole story—more than four in ten sudden unexpected deaths in infancy occur in seemingly healthy babies born full-term. The success of early 20th-century initiatives to reduce infant mortality occurred “before widespread use of vaccination and medical technologies” but instead of learning from history or recognizing the need to avoid exposing young children to unnecessary risks, the U.S. public policy mantra seems to be “full speed ahead.”
Note: For information about infant mortality and the childhood health epidemics get the FREE Children’s Health Defense eBook, “The Sickest Generation: The Facts Behind the Children’s Health Crisis and Why It Needs to End”. The eBook describes how children’s health began to worsen dramatically in the late 1980s following fateful changes in the childhood vaccine schedule in combination with other environmental exposures.
Dr Kohls is a retired family physician from Duluth, MN, USA. Since his retirement from his holistic mental health solo practice, he has been writing weekly columns for northeast Minnesota’s alternative newsweekly magazine, the Duluth Reader. His columns, which are widely re-published around the world, deal with a large variety of justice issues, including the dangers of American fascism (including religious fascism), conscienceless corporatism, militarism, racism, xenophobia, industrial pollution, climate geo-engineering/solar radiation management, the dangers of electromagnetic radiation, Big Copper Mining’s attempts at exploitation of northeast Minnesota’s water-rich environment, Big Medicine’s and Big Pharma’s over-charging, over-screening, over-diagnosing, over-drugging, and over-vaccination agendas, as well as other corporate global movements that threaten human health, the environment, democracy, civility and the sustainability of life on earth. Many of his columns have been archived at a number of websites, including these four: http://duluthreader.com/search?search_term=Duty+to+Warn&p=2; http://www.globalresearch.ca/author/gary-g-kohls; http://freepress.org/geographic-scope/national; and https://www.transcend.org/tms/search/?q=gary+kohls+articles
NOTE: The views expressed here are those of the author and do not necessarily represent or reflect the views of Reader Weekly.”

| Tweet |