News & Articles
Browse all content by date.

“[According to CDC statistics], ‘influenza and pneumonia’ took 62,034 lives in 2001 - 61,777 of which were attributable to pneumonia and 257 to flu, and in only 18 cases was the flu virus positively identified.” – Dr Peter Doshi, from in his 2005 BMJ report, titled, “Are US flu death figures more PR than science?” (BMJ 2005; 331:1412)
“The most lucrative areas of medicine are the most corrupted by financial (and academic) conflicts of interest. So-called ‘authoritative’ sources of medical information are thoroughly corrupted not only by pharmaceutical industry manipulation but also by government officials and financially conflicted academic gatekeepers of medical science, ’expert’ panels, medical journal editors and the largely corrupted vaccine information base.” – Vera Sharav, MD
“For a long time no one considered the effect of repeated vaccinations on the brain. This was based on a mistaken conclusion that the brain was protected from immune activation by its special protective gateway called the blood-brain barrier. More recent studies have shown that immune cells can enter the brain directly, and more importantly, the brain’s own special immune system can be activated by vaccination.” – Russell Blaylock, MD
More important quotes about vaccine effectiveness are at the end of the column (and/or posted at the duluthreader.com
The CDC (the Centers for Disease Control and Prevention) was born, just like the FDA (Food and Drug Administration), as an important regulatory agency of the United States government that was intended to regulate various corrupt and monopoly-seeking industries that could harm the environment and/or the health of individuals and other weaker entities that had no other way to protect themselves from the dangerous practices of any number of powerful industries.
Tragically, over the past couple of generations (particularly since the presidency of Ronald Reagan), both the CDC and the FDA have come under the tight control of many Big Pharma and Big Vaccine corporations (and their Big Bank lenders and lobbying groups) while at the same time abandoning their original charge of protecting the people from the consequences of corporate greed.
The multibillionaire and multimillionaire owners, investors, lobbying groups and think tanks have become grotesquely wealthy and grotesquely powerful because of their ownership and/or investments in a multitude of grotesquely profitable, highly secretive, non-elected and anti-democratic entities that are over-charging for their often toxic and often addictive products that often sicken the users with toxic side effects, drug-drug or vaccine-vaccine interactions, all of which are actually iatrogenic disorders (= doctor- or drug-caused).
The control that those private/corporate/non-elected entities have acquired is easily seen in the day-to-day actions of the corporate-influenced Presidency, the corporate-influenced Congress and the corporate-influenced Supreme Court, all of which seem to be doing the biding of whatever entities will sustain Wall Street’s and War Street’s grotesque profit-making actions.
There should be no surprise why many governmental entities, many of our regulatory agencies, Big Pharma, Big Vaccine, Wall Street, etc have lost a lot of credibility among the populace. But in today’s column I want to focus on the CDC, which annually deals in 4 billion dollar’s worth of vaccines every year and owns dozens of vaccine-related patents that might make the CDC a lot of money in the future.
The CDC is no longer an un-biased entity that is supposed to protect the citizenry from sociopathic corporations. As a matter of fact, the CDC actually acts a lot like such a corporation. A good example is the annual push by the CDC to get everybody in American to get their influenza vaccines, despite the powerful (and often censored-out) evidence that influenza vaccines can be harmful while offering little or no benefit.
One starting point in the debate over the logic of getting annual intramuscular injections of flu vaccines is the reality of Influenza-Like Illnesses (ILI), which comprise 80% of all “flu-like” illnesses that the CDC, Big Medicine and the mainstream media call “the flu” but is actually only “the flu” less than 20% of the time.
ILI is a transient respiratory illness that can be mild, moderate or severe and is usually accompanied by a body temperature (sometimes with chills) greater than 100˚F, a cough and/or sore throat, a runny or stuffy nose, muscle aches, headaches, fatigue and no other known causes for the symptoms. Diarrhea or other gastrointestinal symptoms are not part of an ILI.
ILI is an intermittently-common seasonal syndrome that is best prevented by a combination of good nutrition, good hygiene and avoidance of exposure to virus-shedding individuals. Only in a small minority of instances (see chart below) is the illness prevented by “getting your damn flu shot”.
The actual viruses that cause ILI (usually NOT actual influenza viruses) can only be positively-identified when appropriate costly laboratory tests are done, which doesn’t often happen outside of hospital ER settings because of the high costs. In 2017, Blue Cross reimbursed Medicare $571 (!) for a single Multiplex PCR (Polymerase Chain Reaction) Viral Panel test (CPT code = #87633). Since failure to do a PCR test precludes making a precise diagnosis, the CDC and state Departments of Health take the easy data-gathering route by “assuming” (and then readily publishing) that every ILI is actually a case of influenza! GIGO (Garbage In/Garbage Out)
GIGO: Comparing ILIs (influenza-like illnesses) with MLIs (measles-like illnesses)
The same GIGO reality happens whenever there is a mini-epidemic of any illness that the CDC wants to propagandize. A good example was the “measles” outbreak that happened a few years ago at California’s Disney Land. The cluster of cases was actually a group of “measles-like illnesses” (MLI). PCR tests apparently were not done on all the subjects and so the CDC falsely “assumed” (and then published) that whatever MLIs occurred were “vaccine-preventable” illnesses. PCR tests are not often thoroughly done before the CDC makes use of such propaganda-worthy opportunities that will benefit the CDC and its corporate partners. And the media happily goes along with the charade by over-reporting and over-emphasizing the story.
When PCR studies are actually done in any ILI outbreak, influenza viral infections are usually only identified in less than 25% of patients. The differential diagnosis for ILI syndromes is large. Some of the possibilities, most of which are not even theoretically “vaccine-preventable” – much less medically-treatable - include the following conditions:
Adenovirus, respiratory syncytial virus, human metapneumovirus, HIV, EBV, CMV, viral meningitis or viral or inflammatory encephalitis, West Nile virus, Chickungunya virus, Dengue virus and non-infectious causes such as arthritis, myositis, dermatitis, and oral ulcers.
Of course, no differential diagnostic list on a patient chart is complete until the possible iatrogenic causes of ILI are listed.
Iatrogenic illnesses can be caused by any number of prescription drugs and prescribed vaccines, especially when they are used in drug-drug combinations or vaccine cocktails, none of which have ever been adequately tested for safety or even efficacy.
The potentially toxic ingredients (such as mercury, aluminum, live viruses, etc.) that are in many vaccines are known to actually cause influenza-like symptoms. Here is a list of some of the published adverse effects of typical CDC-approved influenza vaccines:
Headache, fever, nausea, muscle aches, weakness, Guillain-Barre Syndrome, dizzyness, hoarseness, wheezing, hives and soreness, redness, and/or swelling from the shot.”
There are many “white lies” that most “healthcare” reporters tell their readers when their editors order them to help the CDC promote its annual “get your damn flu shot” campaign every fall. Among the many untruths is the lie that 36,000 Americans die of influenza every year. The truth of the matter is that the CDC has always lumped the much larger number of pneumonia deaths with the small number of influenza deaths and then mis-represented the number as influenza deaths!! Just another example of GIGO as investigative reporter Jon Rappaport has written:
“The CDC says that 36,000 people die from the flu every year in the US, but actually, it’s closer to 20. However, we can’t admit that, because if we did, we’d be exposing the (CDC’s) gigantic psy-op. The whole campaign to scare people into getting a flu shot would have about the same effect as warning people to carry iron umbrellas, in case toasters fall out of upper-story windows.”
Another “white lie” that promotes the flu shot campaign is the use of the vaccine efficacy (VE) figure. When such figures are used, percentages like “50% effective” are used to make the vaccine sound good, whereas that number is a miserably low, deceptive “relative risk” figure. Big Pharma corporations, sociopathic entities that they are, always use RRR when they want to make a new drug sound far more effective to its physician-prescribers than it actually is.
Check out this common subterfuge by reading an article that I wrote on the subject at: http://vaccineimpact.com/2018/mercks-fosamax-fraud-demonstrates-how-big-pharma-and-cdc-spin-statistics-to-sell-ineffective-vaccines-and-drugs/
In that article I revealed how Big Pharma’s common use of the relative risk reduction (RRR) allowed Merck to fooled everybody – especially us physicians - by claiming that their block-buster osteoporosis drug Fosamax (and probably all the “me-too” drugs as well) was 50% effective (an RRR statistic) in reducing bone fractures.
However, in Merck’s own raw statistics, it was clear that patients who took the drug for 4 years actually had a miniscule 1-2% absolute risk reduction (AAR) in the incidence of fractures. The 1-2% figure, which would have sunk the product (and the related bone density screening industry) if it was ever revealed, is actually a negative number, especially when the high cost of the drug and its unadvertised risks are considered - such as the incurable, iatrogenic, Fosamax-induced, disastrous osteonecrosis of the jaw.
The most important white lie that is told to us naïve consumers of vaccines is actually the censored-out facts about how the ingredients of America’s annual flu vaccine are chosen. A committee of the CDC meets every early spring to look at the strains of influenza that were most commonly identified in Australia’s “flu season” the year before (the southern hemisphere’s winter flu season occurs during our northern hemisphere’s summer season). The unproven supposition is that the flu viruses that infected Australians the year before will be the same ones that we Americans will be facing. Then samples of the 3 or 4 live influenza viruses most likely to be epidemic (out of over 100 known viruses that could have been chosen) will be collected and grown in Big Vaccine’s chicken egg labs until enough of the viruses is obtained and then added to the toxic brew that will be included -with finger’s crossed - in next fall’s vaccine vials. Of course, there is never any assurance to potential vaccines that there will be a match. In fact, the odds are against any match in any given year.
So I suppose the lesson to any given patient or parent of a potential vaccine (or a physician, nurse practitioner or nurse) is to know everything possible about the actual risks and benefits of any intramuscular vaccination by studying the information above and below before going to the pharmacy or clinic and offering your arm (or thigh, in the case of small infants).
Definitions (from GGK):
Vaccine efficacy (VE) is the percentage reduction in a particular disease outcome in vaccinated compared to unvaccinated individuals. (For example, a VE of 60% means that vaccinated people have a 60% (relative) reduction in their risk of a given outcome compared to unvaccinated people. Ex: After last year’s flu season was over, the VE for flu shots was calculated in one study as being a miserable 9%, and that is a relative risk reduction figure.!
The Number Needed to Vaccinate (NNV) is the number of individuals that must be vaccinated for an expected benefit to be attained in one individual. Mathematically, the NNV is expressed as a ratio of 1 divided by the Absolute Risk Reduction (ARR).
The very similar Number Needed to Treat (NNT) is the number of individuals that must be treated with a drug or surgery that results in benefit to one individual. It is the inverse of ARR. The larger the NNV (or NNT) is, the more useless is the vaccine (or drug).
The Absolute Risk Reduction (ARR) signifies the true difference in the reduction in risk between unvaccinated (or untreated) and vaccinated (or treated) individuals. (The ARR is vastly more meaningful than the widely used and very deceptive Relative Risk Reduction [RRR] figure., which is seriously deceptive.)
More helpful information:
From the American Academy of Pediatrics journal Pediatrics - September 2014, Volume 134 / Issue 3
Severe Complications in
Influenza-like Illnesses
By Rakesh D. Mistry, Jason B. Fischer, Priya A. Prasad, Susan E. Coffin, Elizabeth R. Alpern
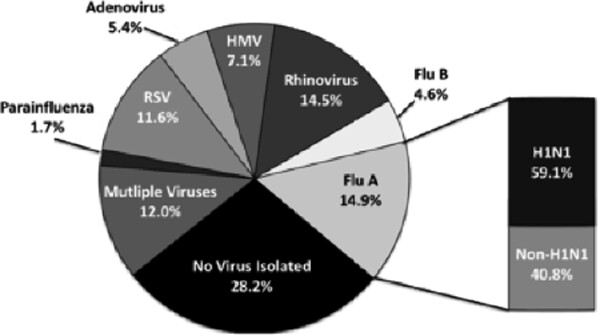
Below is a pie graph depicting the PCR results that were published in the above journal article about Influenza-like Illnesses. Note that actual influenza was only diagnosed in 19% of the patients represented in the graph:
Only 19% of the patients with “influenza-like illnesses” in the study actually had influenza. Interestingly, 57% of the patients with actual influenza had had their routine seasonal influenza vaccinations but had not been protected by the shot.
55% of the study patients that had influenza-like illnesses (but not actual influenza) had likewise not been protected by the flu shot. And of course, every person in the above study that had been intramuscularly-injected with the vaccine could have suffered significant adverse effects.
From the medical journal PLOS One (Published: January 27, 2017)
Influenza Vaccination of Healthcare Workers: Critical Analysis
Gaston De Serres, et al
Background
…We critique and quantify the cRCT evidence for indirect patient benefit underpinning policies of mandatory Health Care Workers (HCW) influenza vaccination.
Methods
…The number needed to vaccinate (NNV) for HCWs to indirectly prevent patient death was recalibrated based on real patient data of hospital-acquired influenza, with adjustment for potential under-detection (5.2-fold) and using favourable assumptions of HCW-attributable risk (ranging 60–80%).
Results
“6000 to 32,000 hospital workers would need to be vaccinated (with an influenza vaccine) before a single patient death could potentially be averted”
Conclusions
…The impression that unvaccinated HCWs place their patients at great influenza peril is exaggerated. …current scientific data are inadequate to support the ethical implementation of enforced HCW influenza vaccination, they do not refute approaches to support voluntary vaccination or other more broadly protective practices, such as staying home or masking when acutely ill.
Based on these data…the NNV would be higher with lower VE or lower HCW-attributable risk. If instead of 60%, the VE in HCWs was assumed to be 40% or less as reported by several studies in Canada and the US for the 2010–11 season, the NNV would increase to at least 54,193 and 61,111, respectively.
Even allowing that as much as 80% of hospital-acquired influenza deaths were due to HCWs, the NNV in hospitals would still range between 24,516 (Canadian network) and 24,614 (US network) for a VE of 60%, and between 40,645 and 45,833 for a VE of 40%.
Applying the highest adjustment factor for under-detection of influenza reported by Reed et al for elderly patients admitted to the US hospital network in 2010–11, the NNV would still range between 6,286 and 6,311 for a VE of 60% and between 10,241 and 11,752 for a VE of 40%.
Following publication of the PLOS ONE journal article, the lead author of the study, Dr. Gaston de Serres was quoted as saying: “I think the bottom line of our paper is to say there is no valid scientific evidence, even now, underpinning enforced health care worker immunizations (with influenza vaccines).” De Serres further said: “… it’s one thing to say: ‘OK, on a voluntary basis, you get the (influenza) vaccine despite all its weaknesses,’ and it’s another thing to say, ‘If you don’t get it, you get fired’.”
Typical for many medical journals these days are these Conflicts of Interests of four of the co-authors of the above journal article:
Gaston De Serres has received grants from GSK and Pfizer and travel reimbursement to attend an ad hoc advisory board meeting of GSK.
Brian J Ward has participated in clinical trials and ad hoc advisory boards with several vaccine manufacturers as well as receiving occasional speaker’s fees. He has held or holds research grants with GSK and Medicago. He is medical officer for Medicago Inc. and has served as an expert witness for US and Quebec vaccine injury compensation programs.
Mel Krajden has received research grants from Roche, Merck, Siemens, Hologic, and Boerhinger Ingelheim for unrelated studies.
Fabrice Carrat has received personal fees from AstraZeneca and GlaxoSmithKline for consultancy on influenza epidemiology outside the submitted work.
More important quotes concerning the NNV (Numbers Needed to Vaccinate):
“I predict that (Merck’s) Gardasil will become the greatest medical scandal of all time because at some point in time, the evidence will add up to prove that this vaccine, technical and scientific feat that it may be, has absolutely no effect on cervical cancer and that all the very many adverse effects which destroy lives and even kill, serve no other purpose than to generate profits for the manufacturers. Gardasil is useless, and it costs a fortune!” -- Dr Bernard Dalbergue (former Merck employee)
“There are only 30 to 40 cervical cancer cases per year per one million (American) women between the ages of 9 and 26. Therefore, you would have to vaccinate (with Gardasil) one million girls to prevent cervical cancer in 4 to 5 girls; and since only 1/3 of of women who develop cervical cancer actually die from the disease, you would have to vaccinate one million girls to prevent 1 to 2 deaths per year - at the “bargain-basement price” of $360 million per year.” – Joseph Mercola, DO
“Assuming that the (Gardasil) vaccine procures lifelong protection and that vaccine efficacy is 95% (both irrationally over-optimistic assumptions!) and if vaccine protection is assumed to wane at 3% per year (also an over-optimistic estimate), the predicted number needed to vaccinate (NNV) would increase to 9,080 (ie you would have to vaccinate 9,080 girls to prevent one case of cervical cancer).” – Summarizing one of the conclusions of a Canadian Medical Association Journal article, 3 of the authors of which had financial conflicts of interest with Merck & Co, the makers of Gardasil. The article--- can be accessed at: www.cmaj.ca/cgi/content/full/177/5/464/DC1
“To spare one person a heart attack, 100 people had to take Lipitor for more than three years, and for every 10 patients taking a statin drug such as Lipitor for 5 years, one of them will develop statin-induced myonecrosis.” (That is, 100 is the NNT for Lipitor to prevent one heart attack after taking the drug for > 3 years and it is 10 for those patients who take a statin for 5 years.) -- (Summary of data from: http://www.thennt.com/nnt/statins-for-heart-disease-prevention-without-prior-heart-disease/)
“The NNV for Prevnar-13 to prevent one case of invasive pneumonia in low-risk asthmatic adults is estimated to be as high as 1059.” (That is 1059 low risk asthmatic adults would have to be vaccinated with Prevnar-13 to prevent invasive pneumonia in one of them.) --https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4173976/

| Tweet |